Clinical Differential Diagnosis
UTI/pyelonephritis, urolithiasis, pancreatitis, neoplasia, IBD, infectious disease.
Image Interpretation
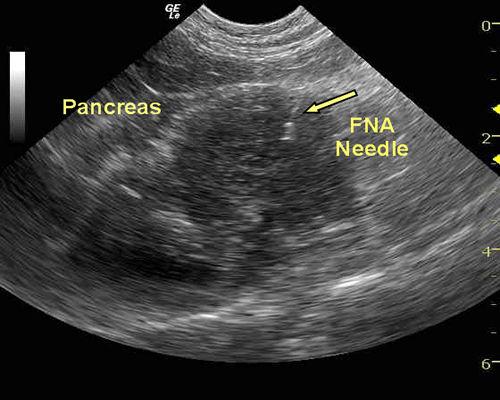
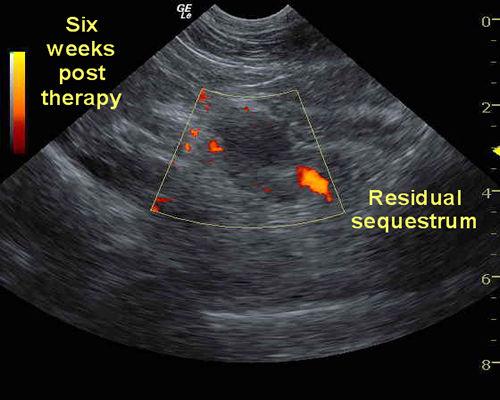
Image 1: A well-circumscribed, hypoechoic mass positioned within the region of the body of the pancreas. Image 2: The mesentery and omentum boarding the pancreas is mildly echogenic and may be adhered. The echogenic linear focus at the 1 o'clock position represents a 22-gauge needle.
Sonographic Differential Diagnosis
Suspect chronic pancreatitis with mild peri-pancratic fibrosis, inflammation and adhesions with an accompanying avascular mass. Differentials for the mass include abscessing or necrotizing neoplasm or focal pancreatitis, sequestration.
Sampling
22g US-guided FNA was performed on variable hypoechoic portions of the pancreas. Cytology: Marked pancreatitis/steatitis/necrosis. No evidence of neoplasia was found.
Outcome
Bartonella henselae. The patient has been thriving for over a year but did recently have a similar but less dramatic clinical presentation that responded to hospitalization and similar treatment.


Comments